- Anesthesiologist specializing in non-surgical spine care
Fellowship-trained in Interventional Spine
Spondylolysis
Overview | Causes | Symptoms | Diagnosis | Treatment | FAQ
Overview
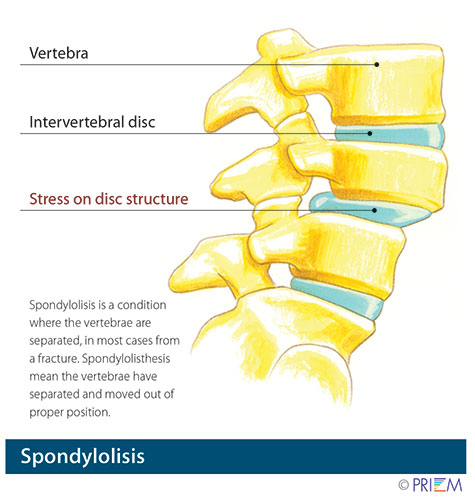
Spondylolysis relates to instability of specific bones in the low back.
It a very common cause of back pain, particularly in adolescents.
Gymnasts who perform routines that bend and arch the back are often
victims of spondylolysis or spondylolisthesis.
[top]
Click on image to enlarge
Causes
Spondylolisthesis and spondylolysis are caused by joint instability
in the low back. The rear part of spinal vertebrae has facet joints
that act as hinges, allowing our spines to twist and bend. Sometimes,
however, the posterior element can crack. Either from heredity or
wear and tear, part of the posterior element called the pars interarticularis
can crack, causing the vertebrae slip forward out of its correct
position. Spondylolysis occurs when the PARS hinge is cracked, but
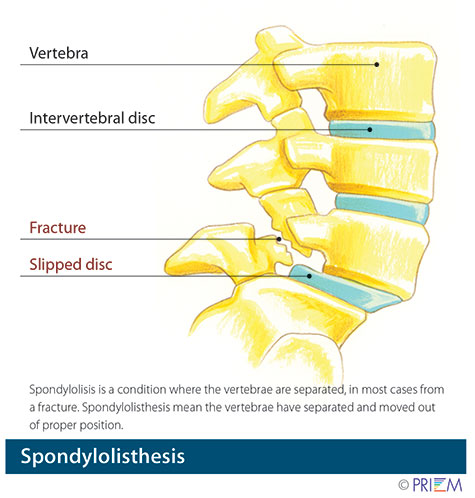
the vertebrae is still in its correct position. Spondylolisthesis
occurs when the cracked PARS has allowed the vertebrae to slide forward
out of its correct position. If left untreated, spondylolysis can
lead to spondylolisthesis.
[top]
Symptoms
Interestingly, in many cases, spondylolisthesis may have no symptoms,
so most people may not know they have it. Back pain is the most common
symptom, particularly in the lower back. This back pain may be mistaken
for a muscle strain. Muscle spasms that occur as a result of spondylolysis
may cause an overall feeling of stiffness in the back and may effect
posture.
[top]
Click on image to enlarge
Diagnosis
Outlined below are some of the diagnostic tools that your physician may use to gain insight into your condition and determine the best treatment plan for your condition.
Medical history: Conducting a detailed medical history helps the doctor better understand the possible causes of your back and neck pain which can help outline the most appropriate treatment.
Physical exam: During the physical exam, your physician will try to pinpoint the source of pain. Simple tests for flexibility and muscle strength may also be conducted.
X-rays are usually the first step in diagnostic testing methods. X-rays show bones and the space between bones. They are of limited value, however, since they do not show muscles and ligaments.
MRI (magnetic resonance imaging) uses a magnetic field and radio waves to generate highly detailed pictures of the inside of your body. Since X-rays only show bones, MRIs are needed to visualize soft tissues like discs in the spine. This type of imaging is very safe and usually pain-free.
CT scan/myelogram: A CT scan is similar to an MRI in that it provides diagnostic information about the internal structures of the spine. A myelogram is used to diagnose a bulging disc, tumor, or changes in the bones surrounding the spinal cord or nerves. A local anesthetic is injected into the low back to numb the area. A lumbar puncture (spinal tap) is then performed. A dye is injected into the spinal canal to reveal where problems lie.
Electrodiagnostics: Electrical testing of the nerves and spinal cord may be performed as part of a diagnostic workup. These tests, called electromyography (EMG) or somato sensory evoked potentials (SSEP), assist your doctor in understanding how your nerves or spinal cord are affected by your condition.
Bone scan: Bone imaging is used to detect infection, malignancy, fractures and arthritis in any part of the skeleton. Bone scans are also used for finding lesions for biopsy or excision.
Discography is used to determine the internal structure of a disc. It is performed by using a local anesthetic and injecting a dye into the disc under X-ray guidance. An X-ray and CT scan are performed to view the disc composition to determine if its structure is normal or abnormal. In addition to the disc appearance, your doctor will note any pain associated with this injection. The benefit of a discogram is that it enables the physician to confirm the disc level that is causing your pain. This ensures that surgery will be more successful and reduces the risk of operating on the wrong disc.
Injections: Pain-relieving injections can relieve back pain and give the physician important information about your problem, as well as provide a bridge therapy.
[top]
Treatment
Conservative treatments should always be considered first when treating
spondylolysis. Nonsurgical treatment methods include resting and
refraining from usual activities, taking anti-inflammatory medication,
and incorporating a stretching and strengthening program. While ligaments
and muscles can help hold the vertebrae in place, over time, surgery
may be necessary to install surgical instrumentation or bone grafts
that lock the vertebra in place so that it does not slide out of
position and damage the spinal nerves. Surgery may involve a fusion
and/or screws and rods.
[top]
FAQs
How do I know if I am at risk for spondylolysis?
Those with a family history of spondylolysis or weak vertebrae are
more susceptible to developing the condition. Also, athletes involved
in activities that place a great deal of stress on the back, such as
football players and weight lifters, are at greater risk for fracturing
the vertebrae, encouraging slippage.
[top]
Disclaimer:
The pictures displayed in Baptist Health Spine Center are images of physicians, patients and employees who have consented to have their pictures in this website. If you are viewing in Internet Explorer 8 or older you may need to update your browser by clicking here.
Non-surgical Spine Care
-
 Andrew Gunter Cain, MD
Andrew Gunter Cain, MD
Affiliated Spine Surgeons
can be reached at 501-224-0200
-
 Tim Burson, MD
Tim Burson, MD- Board-Certified
Neurological Surgeon
- Board-Certified
-

-

-
 Blake Phillips, MD
Blake Phillips, MD- Board-Certified
Neurological Surgeon
- Board-Certified
-
 Jonathan Reding, MD
Jonathan Reding, MD- Board-Certified
Neurological Surgeon
Fellowship-Trained Neurosurgeon
- Board-Certified
Back to Life Journal

Home Remedy Book